
A huge antibody response to prolonged antigen presentation from mRNA-produced spike proteins induces long-term IgG4 autoimmunity in those who were vaccinated with mRNA vaccines and lacked previous exposure to SARS-CoV-2. This problem has not been observed in other types of Covid-19 vaccines. Data from Kiszel et al (2023).
I’ve previously discussed the poor design and manufacturing of mRNA vaccines for Covid-19, how they have injured people, and proposed a better means to produce these vaccines. More evidence has recently emerged describing how these mRNA vaccines may be causing injuries through autoantibody activation. Let’s briefly look at the recent paper of Kiszel et al, 2023.
The most abundant antibody (also called immunoglobulin) isotype in the human serum (blood is different from mucosa where IgA dominates) is immunoglobulin G (IgG). The subclasses of IgG are very similar but differ in their constant regions (the region of antibody used to destroy antigens). Each subclass has a unique profile in terms of antigen binding, immune complex formation, complement activation and triggering of effector cell activation. After antigenic stimuli, IgG3 and IgG1, the two main complement-activating subclasses are secreted first, whereas IgG2 and IgG4, which are formed later, are thought to play a role in attenuating inflammation due to their inability to activate complement. Previous studies have found that antibody responses to viral protein antigens are mainly restricted to IgG1 and IgG3. IgG2 is stimulated primarily by carbohydrate antigens, whereas IgG4 is produced in response to helminthic (parasitic worms) infections or to, very importantly to mechanisms of action in mRNA vaccine injury, prolonged antigen stimulations. mRNA vaccination yields a higher antibody titer than does the SARS-CoV-2 infection. In other words, a huge amount of antigen presentation elicited by the mRNA vaccination induces a huge amount of antibody production – too much. That huge antibody production means a high level of autoantibodies, such as IgG4.
IgG4 can mediate autoimmune diseases. However, IgG subclasses produced against protein antigens depend on factors other than the type of pathogens or type of vaccine, such as T-helper cell response, and the route and the site of infections or injections. As such, the intricacies of how an individual will respond to a particular vaccine is largely unknown. The drug companies don’t want to know because their business model is to give a drug to as many people as possible, and knowing about injuries is an impediment to making money. Leave it to academic researchers who aren’t paid-off by pharma to figure out the safety data. Alas, there is not enough money in academia to do this well, but Kiszel et al (2023) give us important info.
Now let’s look at what mRNA vaccines do to the different antibody levels. Here’s Figure 5 from Kiszel et al (2023).
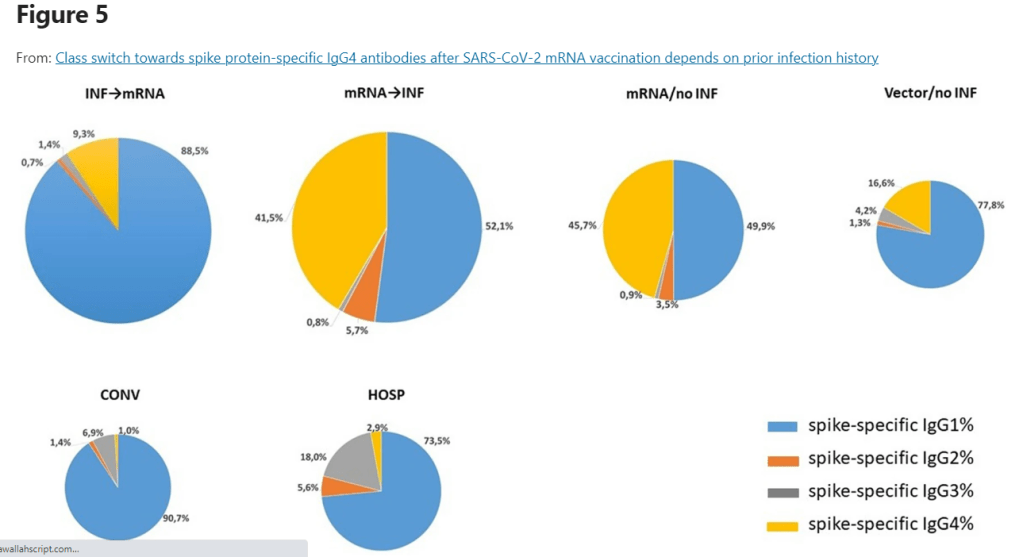

Notice that the percentages of spike-specific IgG4 were higher in the vaccinated groups than in the COVID-19 infected groups. The proportions of the spike-specific IgG4 subclass to the sum of all spike-specific IgG antibodies were between 1 and 3% in the infected groups. However, in the vaccinated groups, they detected 16.6% of spike-specific IgG4 in the Vector/no INF group, whereas its values were as high as 41.5% and 45.7% in the mRNA → INF and mRNA/no INF groups, respectively. That is, those who were mRNA-vaccinated but had no previous Covid-19 infection (mRNA –>INF) or who had no Covid-19 infection before or after vaccination (no INF), had high levels of IgG4.
The bottom line is that the Covid-19 mRNA vaccines are poor vaccines that injure many people, don’t stop or reduce transmission, and must be given every 6 months. Increased levels of IgG4 autoantibodies following mRNA Covid-19 vaccination is one reason people are injured. This is a big money maker for drug companies that make the vaccines and the drugs used to treat the symptoms of the vaccine injury, such as Rituximab (something that is expensive, has to be administered IV every 6 months, and has many negative side-effects), and is also a money-maker for physicians who often administer vaccines and perform the treatments of those that they have injured with these poor vaccines.
A better choice is to avoid mRNA vaccines, wear a mask, and if you are injured by the mRNA Covid-19 vaccine, choose a diet and exercise plan to limit the severity of the disease.
