The US now lives in the era of short-term monetization research led by billionaires, instead of the long-term innovation paradigm led by our non-profit academic research institutions. VC-backed AI startups reflect this shift as the US loses its lead in almost all aspects of science and engineering to China.
Typical in empires that have reached their final phase of collapse, the so-called decadence phase followed by collapse, money accumulates in a few people and the middle class is obliterated, innovative research at the universities is chopped, domestic policies become militaristic, wars are waged on many other countries, and another country takes over as the lead state when the empire collapses. As billions are spent in the USA on AI companies that make a few new billionaires and makes exisitng billionaires richer, it doesn’t make great AI. Instead, a young Chinese computer scientist, Liang Wenfeng, with BS and MS degrees from the prestigious Zhejiang University in the great tech city of Hangzhou, in the province of Zhejiang, using thousands of dollars, not billions of dollars, developed an AI frontier platform, DeepSeek, that is as good as ChatGPT and 95% less expensive. And, it’s open source , what OpenAI was supposed to be until the greedy Sam Altman, a college dropout and Snake Oil Salesman, decided he wanted to be a billionaire and made OpenAI just more of the same. Little wonder the cofounder of OpenAI, Dr. John Schulman, PhD, who developed its technology, left OpenAI (Schulman talks about how AI convincingly makes things up, AKA, spews BS, here). Yes, the US is in the midst of a great AI Snake Oil boom. Both the AI CEOs and their AI platforms spew BS. And, yes, bullshit is an AI technical term. While AI is great, and I’ve personally worked on biological cybernetics much of my life, the snake oil, overhype and plutocratization is not.
The age of decadence and collapsein the USA is upon us. Capital, the output of US workers, is being used to fund the whims of US billionaires. Sam Altman uses the people’s capital to give more than a billion dollars to a startup to improve longevity. RetroBio is a company led by a guy who’s had 3 venture-backed startups. Start something, pump it, and dump it. Instead of capital flowing to serious scientists at nearby UC Berkeley, UCSF, and Stanford, the money flows to the short-term looking venture company, the longevity company de jour, promising you youth. Instead of buying the Blue Zones Cookbook and taking control of your health, they want to use irradiation and/or chemo to remove your bone marrow cells, and then replace the cells with genetically or epigentically (it’s not clear from their website what they’ll do; remember, Muskian hyperbole is short on specifics, but long on grandiose recycled sci-fi stories) reprogrammed bone marrow cells. Such procedures typically mean the patient is irradiated, resulting in long term toxicity that may include cognitive deficits, cataracts, pituitary dysfunction, gonadal failure, hypothyroidism, cardiac dysfunction, xerostomia, osteopenia, dental complications, chronic kidney disease and secondary malignancies. And once you’ve been irradiated into an unhealthy state and seek health care, the AI company in Tennessee, naviHealth, will analyze you with its algorithm (nH Predict) that is tuned to deny you any healthcare. So efficient is nH Predict, it denied more than 300,000 claims in a two-month period, which amounts to about 1.2 seconds for each physician-reviewed claim. Optum Health , part of United Health Group, Luigi’s favorite company, owns this AI company.
Once the billionaires have irradiated you and induced a 300 year long state of dementia in you, you’ll be dumb enough to jump on one of Elon Musk’s exploding Starships (7 so far; remember during the golden age of science and engineering in the USA when NASA was lead by a doctor of science and the Saturn project never had an exploding rocket and on mission #5 men were on the moon) for a ride to Mars. And don’t forget to have your blood tested to make sure you’re ready to go. Houstonian, daughter of an Enron executive, Elizabeth Holmes, another college dropout, has the best test for your blood with her Theranos start-up technology. AI physicians will then give you your prescription Alzheimer drugs for your trip to Mars. The irradiation you had at RetroBio will induce cognitive decline, and the drug is sure to help. The drug was “developed” by Vivek Ramaswamy at his Bermumda-based startup drug company, Roivant (ROI=return on investment), and made Vivek a multi-millionaire. Too bad it was all a scam. Once you’re on Mars, you’ll likely want to jump on Musk’s Hyperloop for a view of his vast colonization project, replete with Musk’s solar panel system, the best in the universe. Enjoy living to be 300 years old, stultified, and demented in your Mars cell. You’re living insel-Musk’s wet dream.
Please enjoy your billionaire led government, and, remember, don’t question authority and believe the hyperbole of a bunch of short-term thinking college dropouts. All will be well as you live to 300 years old in your cell on Mars counting your crypto meme coins and watching Nazi salutes on Twitter, the only media available on Mars, as Musk hangs-out in his compound with his 12 wives and 52 children, never having flown in a Starship. Sam Altman will say every year that AI will, in the next two years, do everything humans do, the RetroBio guy will be on his 100th startup, and Trump will still be President of what’s left of the USA.
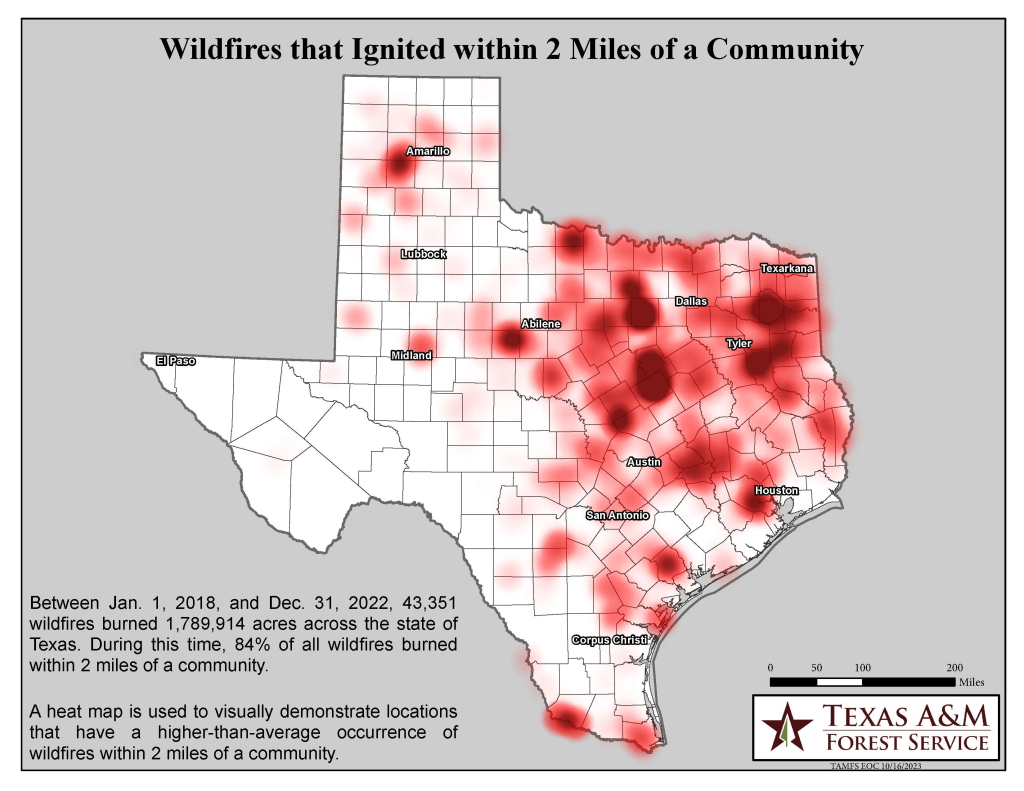
Considering the three largest states in the USA, California, Texas, and Florida, it is California that has the least number of disasters with the lowest cost burden, by far, of the three. Texas, of course, is the number one disaster state. Yet, when the state of California faces a disaster, Republican politicians, especially those from Texas, immediately weigh-in to criticize the state and threaten, and actually vote for, withholding federal money to prevent and remediate the disasters. When Red States face disaster, Democrats don’t play political games – relief is offered immediately. It is as if Republicans relish disasters so that they can selectively call-out California, but on the other hand lack introspection to see their regressive policies actually are hurting their own Red States more than the Blue States. It makes for great political theatre, though, and mainstream media gives these regressive Republican clowns the theatre they don’t deserve.So, Texas is the #1 disaster state, and also number one in trying to withhold disaster relief from Blue States.
In 2024 alone, one wildfire in Texas burned over 1 million acres. Between 2018-2022, about 1.8 million acres were burned by wildfires in Texas. Unlike what Republicans do, Democrats didn’t withold, or threaten to withold, disaster relief to Texas.
Although the flames that leveled Pacific Palisades and Malibu are believed to have started in the Santa Monica Mountains National Recreation Area, managed by the National Park Service, and the blaze that turned Altadena to ash burned through the Angeles National Forest, is managed by the U.S. Forest Service, which is part of the United States Department of Agriculture, Republicans blame California for the fires. Republicans have continuously gutted funding to US land management and have privatized as much of it as they can. Republicans create problems and then blame others for the problems.
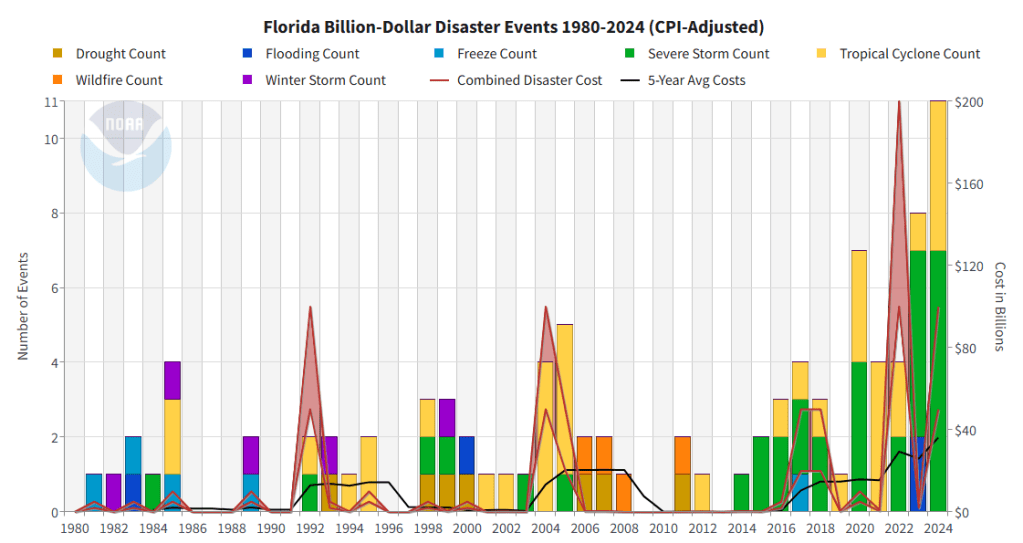
From 1980–2024, there were 94 confirmed weather/climate disaster events with losses exceeding $1 billion each to affect Florida. These events included 7 drought events, 4 flooding events, 5 freeze events, 33 severe storm events, 36 tropical cyclone events, 4 wildfire events, and 5 winter storm events. The 1980–2024 annual average is 2.1 events (CPI-adjusted); the annual average for the most recent 5 years (2020–2024) is 6.8 events (CPI-adjusted).
California Summary
From 1980–2024, there were 46 confirmed weather/climate disaster events with losses exceeding $1 billion each to affect California. These events included 14 drought events, 6 flooding events, 3 freeze events, 4 severe storm events, and 19 wildfire events. The 1980–2024 annual average is 1.0 event (CPI-adjusted); the annual average for the most recent 5 years (2020–2024) is 1.6 events (CPI-adjusted).
Texas Summary
From 1980–2024, there were 190 confirmed weather/climate disaster events with losses exceeding $1 billion each to affect Texas. These events included 20 drought events, 9 flooding events, 1 freeze event, 126 severe storm events, 16 tropical cyclone events, 7 wildfire events, and 11 winter storm events. The 1980–2024 annual average is 4.2 events (CPI-adjusted); the annual average for the most recent 5 years (2020–2024) is 13.6 events (CPI-adjusted).
We now live in the age of renewable energy, although big oil and their political shills will argue otherwise through their lies. President Jimmy Carter’s lead in renewable energy, especially solar energy, was quashed by the regressive policies of Ronald Reagan, a puppet of the wealthy.
The USS Nautilus, created by Admiral Rickover, BS., M.S., who was trained as an electrical engineer, and with Jimmy Carter, B.S., on board as its chief nuclear engineer.
Jimmy Carter, who died in December 2024 at the age of 100, saved the world in the 1970s. Not only fixing the ozone hole, Carter was a nuclear engineer who trained at the US Naval Academy. The Navy’s work in developing the first nuclear submarine, the USS Nautilus, meant that Admiral Rickover and Jimmy Carter, who was the head nuclear engineer on board, had access to the latest in top-secret nuclear energy technology. When Canada’s Chalk River nuclear research facility experienced a power surge that damaged its reactor, the U.S. sent Carter and his team to fix it. He was one of a few people in the world with the knowledge and skills to carry-out the mission. Fuel rods at the research reactor experienced a partial meltdown after the power surge. It ruptured the reactor and flooded the facility’s basement with radioactive water, rendering the reactor core unusable. Besides many of his accomplishments as President, including the Camp David Accords, the Panama Canal Treaties, and the second round of Strategic Arms Limitation Talks, he also confronted stagflation inherited from Nixon/Ford by appointing Paul Volcker as Fed Chair who was kept on by Reagan and who would end the financial crisis. He signed into law bills that established the United States Department of Energy and the United States Department of Education, and he saved the hostages in Iran (although a treasonous Ronald Reagan took credit for this).
However, his criticism of Israel and its settlements on Palestinian land likely cost him his reelection. Carter’s calling out Israel as an apartheid state riled many Zionist Jews and those who are paid-off by AIPAC. Zionist controls of the media are present too, thus amplifying criticism of people such as Carter who dare to question Israel. The Zionist Jews are powerful and can destroy progressive candidates. They were a factor in eliminating Carter.
Carter was a visonary leader who promoted renewable energy and conservation, including:
National Energy Plan: Carter’s plan included new laws and regulations to promote energy efficiency and conservation, and to develop alternative energy technologies.
Solar panels on the White House: In 1979, Carter installed 32 solar thermal panels on the White House.
National Energy Act: In 1978, Carter introduced the National Energy Act, which set goals to reduce the country’s reliance on oil and increase the use of renewable resources.
Solar bank: Carter proposed spending $100 million in 1980 to create a solar bank, and asked for additional funds to support solar research and projects.
Tax credits: Carter offered $1 billion in tax credits to homeowners who installed solar panels or wind-energy systems.
Sun Day: Carter declared May 3, 1978 to be Sun Day, and gave a speech at a solar-research facility in Golden, Colorado.
Department of Energy: Carter signed legislation in 1977 to create the U.S. Department of Energy
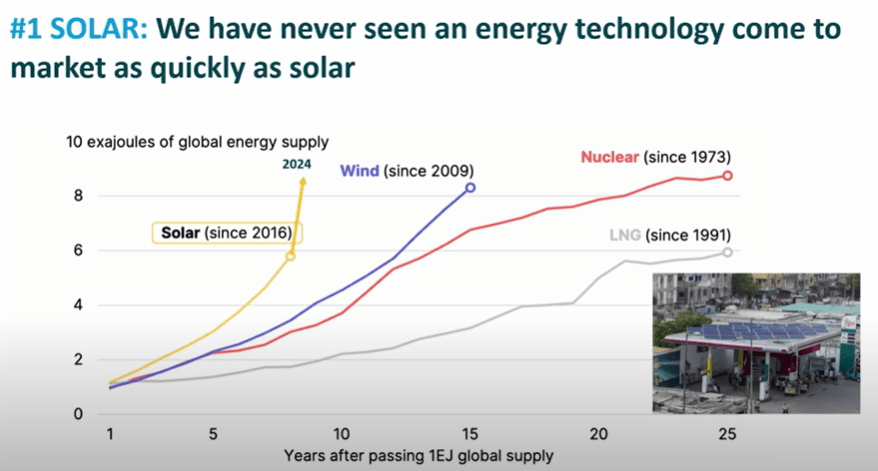
Solar cells had been invented in the USA, and in the 1970s, the USA was the leader in the technology. Carter understood, use solar cells to power things, importantly, to power batteries, and you’ve got an energy revolution. A renewable energy revolution.
First, solar has quickly gone to market and now makes as much energy as does nuclear.
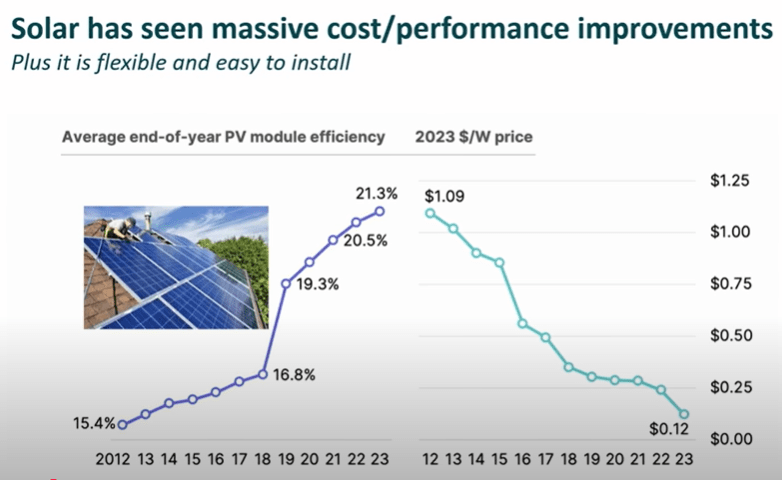
Second, solar is efficient and therefore inexpensive.
Lithium-ion batteries, also invented in the USA, provide storage for the solar energy so it can be used when the sun stops shining. The green area is where the batteries come into play.
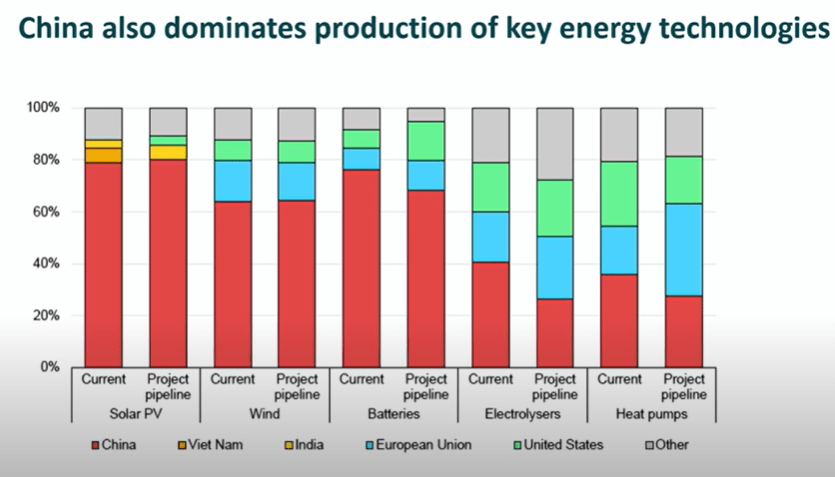
China now leads the USA in financing renewable energy. Unfortuantely, the USA didn’t follow Carter’s lead, but the Chinese did.
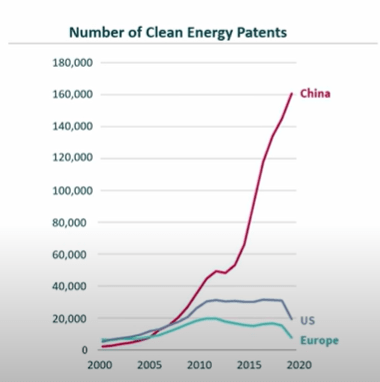
China leads in all other renewable energy technologies.
China has overtaken the USA in developing new renewable energy technologies.
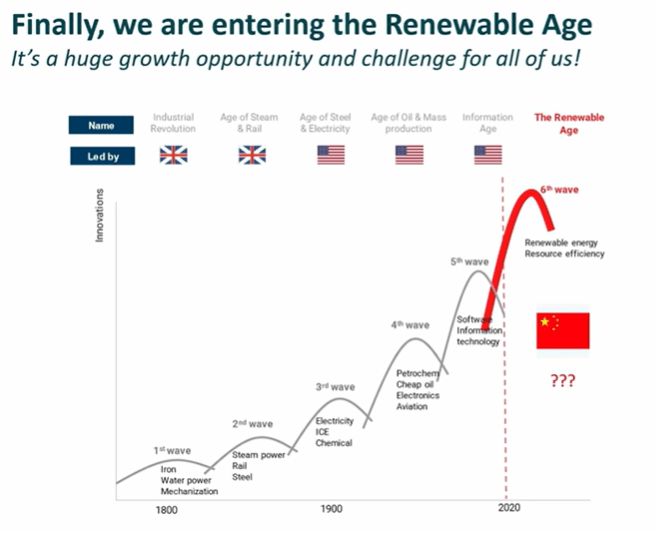
For the last 100 years the USA has lead the various technology revolutions. However we passed the lead to China when we consider the new era of renewable energies.
Like his Cybertruck, Robotaxi, Tesla Semi, Tesla Roadster, Solar Panels, Hyperloop, Exploding Starships, Boring Company, Musk’s genius spending bill idea crashed and burned. Now he’s doing a media blitz so as not to be blamed, including by Trump.
Elon Musk, who didn’t found Tesla, but stole it from the founders, and co-founded SpaceX but didn’t create any of its technology – Tom Mueller did, is hoping to dispel the widely circulating notion that he, a78 year old buffoon who Musk paid to elect, warmongering President-elect Trump, is really calling the shots. Musk is quickly doing what he can to make people forget his failed attempt to sway the US legislation. “No bills should be passed Congress until Jan 20, when @realDonaldTrump takes office. None. Zero,” Musk wrote in a separate post, which read like marching orders to the more sycophantic GOP members, some of whom began to fantasize about a Congress led by Musk himself. Yes, “dipshits” in the Billionaire’s Party have been calling for the depressed Ketamine Kid to be Stutterer [Speaker] of the House.
On Thursday, Twitter user Lulu Cheng Meservey called these proclamations that Trump is not in charge, indicative of a wider strategy to foment discord between the Ketamine Kid and Trump. “By jabbing Trump about not being the alpha, the idea is to provoke him to sideline Elon and to fray the relationship,” Lulu-the-Lemon wrote. Musk, raised by an abusive father who is so disgusting that he had a child with his stepdaughter, is in constant yearning of approval having never had paternal approval during his critical period, leading to his emotional instability and need to control people and impregnate as many women as possible.
Musk, who spends most of his time on Twitter espousing exxtreme-right-wing nonsense that benfits him, agreed, writing in a quote-tweet Friday, “The political & legacy media puppets all got their new instructions yesterday and are now parroting the same message to drive a wedge between [Trump] and me. They will fail.”
The “President Musk” rhetoric began after the stuttering insel, an apartheid-loving South African whose father enslaved black people in emerald mines, and whose financial support for Trump and other Republican candidates made him 2024’s biggest political donor, helped tank a bipartisan spending bill that was brough to vote in the House. Musk unleashed a fusillade of criticism on his social media platform, Twitter, as well as a threat to fund primary challenges against representatives who voted to pass the deal.
Later that day, President-elect Trump, following Musk’s directives, came out against the deal, and after a failed vote on a revised bill Thursday, House Republicans scrambled to put together an eleventh-hour plan to avoid a government shutdown.
Whatever the state of Musk and Trump’s bromance after the world’s wealthiest creep flexed his political muscles this week, the notion that Musk is delivering marching orders seems to have struck a nerve with team Trump. On Thursday, a Trump spokesperson insisted that the president-elect, and no one else, was in charge, saying, “President Trump is the leader of the Republican Party. Full stop.” Actually, it’s the billionaires who own Trump, like Musk and Israeli Zionist Jew, Miriam Adelson, who tell Trump what to do.
A bureaucracy is a system of organization that uses rules and procedures to coordinate the work of many people to accomplish large-scale tasks. Bureaucracies are often characterized by:
Hierarchy: A system of authority with levels of responsibility
Specialization: Individuals are assigned specific tasks
Impersonality: Rules are applied without regard to personal circumstances
When oversight of the bureaucracy by the people is in place, the system works well. But put the wealthy in charge of the bureaucracy, then only the wealthy benefit. Beginning in the 1980s under Reagan, the wealthy gained more and more power of the US government. The people suffered. The result, higher taxes on, and fewer benefits for, the middle class. The rich boys benefit. Inefficiency is great – which means the wealthy assholes have more ways to steal money from the middle class. Just ask Elon Musk who so far has blown-up 6 starships, costing taxpayers about $ 4 billion (Remember in the 1960s before Reagan, Saturn-5 put a man on the moon – yes, in just 5 missions with no Saturn rockets blowing-up). Trump brings the penultimate bureaucracy for benefit of his wealthy buddies.
Any middle-class person who voted for Trump is a moron. That is all.
Meet Function Health, an Austin, Texas-based, venture capital-backed company offering gobs of blood tests, all for only $500/year. Wow, what a deal. They even tell you how old you are by analyzing your blood. Theirs is a Theranosesque story of a young woman solving her own health issues who decides to save the world in the process. Acquires venture capital backing and hires a bunch of famous people, along with some quack physicians (Mark Hyman is cofounder), who love money, to become a part of their scam.
The physician behind Functional Health is Mark Hyman (known for his “bullshit”), a promotor of high-fat diets and the ingestion of coconut oil. Some people will do nearly anything for money. Hyman’s diet recommendations that include red meat and coconut oil (contains 92% saturated fat) have been found to be contributors to the epidemic of colorectal cancer. Is Hyman aware that coconut oil ingestion in a high-fat diet produced dysbiosis associated with an increased colorectal cancer risk? Of course not, he’s too busy making videos, selling the supplement du jour, signing bad books (see a review by Dr. T. Colin Campbell of Cornell University), and doing other things to make money. Further, “coconut oil had a greater impact than soy oil on mice lipid metabolism, resulting in a significant increase in plasma total cholesterol and triglycerides. Not surprisingly, since it is widely accepted that saturated fats, unlike unsaturated fats, can raise blood levels of total cholesterol and triglycerides.” Moreover, “The consumption of saturated fatty acids (SFA), the main compound in coconut oil (CO), can promote insulin and leptin resistance and are associated with inflammation and obesity.” Eating a high fat diet not only harms self, so too are your offspring harmed by a high fat diet. Recent studies find immunometabolic changes in bone marrow and myeloid cells of offspring whose mothers had a high fat diet and obesity, leading to an increased later life risk of infection and cancer.
Hyman also recommends a high protein diet. A diet rich in animal proteins can lead to increased production of TMAO from intestinal microbiota, augmenting the risk of cardiovascular disease, while plant-based proteins could positively influence gut microbial homeostasis. The high intake of saturated fats and omega-6 PUFA, and the reduced intake of omega-3 PUFA, typical of a western-type diet and what Hyman is suggesting, could lead to dysbiosis, gut barrier alterations, and metabolic disorders. Hyman, it seems, likes chronic disease – the more sick people, the more money he makes.
Hyman is a social media darling, perfect for VCs who want to make $billions more than they currently have. And like the uneducated tech-bros that they are, they use cool tech-bro terms at Function Health to describe what they do. For instance, “Your Stack developed with top doctors,” using “stack” that is the mantra for tech bros to describe damn near everything these days, having derived from computer technology describing the front end and the back end of computer applications and the term “full stack.” Note that tech-bro insels such as Elon Musk are fully into this terminology as exemplified by a recent tweet on Twitter from Musk:
Function Health Test Results
Let’s have a look at how these people at Functional Health plan to make billions.
LDL-Cholesterol
Someone I know is trying the Functional Health program and recently received their first test results. Here’s the result for LDL-Cholesterol from the person’s blood test.
This person was very concerned because the result said they were “Above Range” for LDL-Cholesterol. Sounds bad, right?
But here’s what Johns Hopkins Medicine says about LDL-Cholesterol:
The LDL cholesterol range for adults is:
Optimal: Less than 100 mg/dL
Near optimal: 100–129 mg/dL
Borderline high: 130–159 mg/dL
High: 160–189 mg/dL
Very high: 190 mg/dL and higher
Wow! LDL cholesterol at 106mg/dl is nearly optimal, hardly the scarry “Above Range” reported by Functional Health.
Apolipoprotein B (ApoB)
Apo B is protein that is primarily found bound to LDL, and high LDL- cholesterol raises the risk for heart disease and stroke because it builds up as plaque on the walls of your blood vessels.
Here’s the result for apoB from the person’s blood test:
This person was very concerned because the result said they were “Above Range” for ApoB. Sounds bad, right?
Here’s what the Cleveland Clinic says about ApoB range:
“What is a normal Apo B level? A normal Apo B level is: 66 to 133 mg/dL for a man or adult assigned male at birth (AMAB).60 to 117 mg/dL for a woman or adult assigned female at birth (AFAB).”
Once again, Wow! What Function Health says in “Above Range” is called normal by the Cleveland Clinic. These people at FH are using scare tactic to suck people in.
Thyroid Test is Offered
Overprecribing thyroid medication is rampant in the USA. According to Yale University School of Medicine, as many as 90 percent of those who take levothyroxine [Synthroid] may have been unnecessarily prescribed the hypothyroidism medication. There’s a natural diurnal variation in TSH (thyroid-stimulating hormone), and the hormone is at its lowest during the working hours. TSH also varies with the season, being highest in winter.
So, think about it. Report to a lab for your blood work during the day, during the summer, when your TSH is at its trough, and guess what? Your thyroid test says you have low TSH when you likely have a normal range of TSH. Next, they’ll likely recommend you take a pill, a thyroid medication.
The same can be said for LDL. LDL cholesterol levels peak in the afternoon, around 14:39–17:29 hours, and coincide with food intake. Yet these morons at Function Health, including their physicians, are ignorant that LDL has significant diurnal variation.
Most of the Western European countries have rejected water fluoridation including Austria, Belgium, Denmark, Finland, France, Germany, Iceland, Italy, Luxembourg, Netherlands, Norway, Sweden, and Switzerland. For good reason. The topical benefits of fluoride for dental caries are as good as systemic but the associated risks are maximal when ingested. The ideal recommendation would be to limit fluoride (or preferably hydroxyapaptite) to topical dentifrices and mouthwashes. Fluoridation of community drinking water supply is an unreasonable risk.
The USA is in the throws of a binary, reactionary dialogue on many issues, including fluoride in our drinking water. While fluoride can prevent, and even remediate dental caries when administered systemically in the drinking water, there are many negative consequences. A recent study revealed that the concentration of fluorine is elevated in the shells of senior nanocrystals relative to young and that the embrittlement of enamel is driven, at least in part, by the infusion of fluorine into the nanocrystals. In other words, as we age and the enamel of our teeth goes through deenamelization and reenamelization processes, fluoride from water and dental products enters the enamel and makes the enamel more brittle and susceptible to cracking. Using hydroxyapatite in our dental products, a normal mineral found in teeth, may not make the enamel more brittle, and therefore less susceptible to cracking. This needs to be tested.
A recent analysis by scientists at the National Toxicology Program of the US-HHS found that, given fluoride in the water negatively affects childrn’s IQ, “More studies are needed to fully understand the potential for lower fluoride exposure to affect children’s IQ.” Better to add fluoride or hydroxyapatite (a natural mineral found in teeth and bone that can remineralize teeth) to toothpaste, for example, than to administer fluoride to the whole body.
The US Center of Disease Control and Prevention declared that in the second half of the 20th century, the steep decline dental decay in the United States can be attributed to fluoridation. However, data have found that a similar decline in dental decay has been observed worldwide in countries that do not fluoridate their drinking water supplies. A 2024 Cochrane review article found that adding fluoride to drinking water may lead to slightly less tooth decay among children, but concluded that the practice’s effects are less dramatic today than they were before fluoride was widely found in toothpaste.
In 2006, a report by the National Research Council (NRC) acknowledged that fluoride exposure may be associated with adverse cognitive and endocrine outcomes, and recommended further study, especially for vulnerable populations. One NRC panel member, Dr. Robert Isaacson, Ph.D., said the report “should be a wake-up call”. Yet, for 10 years, not a single study had directly examined fetal exposure to fluoride in humans. Now studies have been conducted and fluoride has been found not to be safe in our drinking water. Let’s look at some of the evidence.
Fluoride absorbs into bone and is associated with bone cancer and fracture, therefore I recommend hydroxyapatite, and natural mineral found in teeth and bone. Fluoride in the water is associated with compromised bone quality and the interaction between osteoblasts and osteoclasts is altered and may aggravate osteoporosis and increase osteoporotic fractures. Combine fluoride with the highly overpresribed thyroid medication, Levothyroxine, that, according to scientists at Johns Hopkins, may be contributing to osteoporosis, and people, especially with a poor diet, may be losing bone mass and strength.
Once fluoride is added in the water, it is impossible to control the dose each individual receives. This is because some people, for example, manual laborers, athletes, diabetics, and people with kidney disease, drink more water than others. In addition, the average person receives fluoride from sources other than the water supply such as fluoridated oral hygiene products, food, and beverages processed with fluoridated water, mechanically deboned meat, and teas.
Only 50% of the daily ingested fluoride is excreted through the kidneys. The remainder accumulates in bones, the pineal gland, and other tissues. Initial studies on animals showed that fluoride accumulation in the pineal gland led to reduced melatonin production and an earlier onset of puberty. The same researcher then showed in later studies that fluoride can also accumulate to very high levels in the human pineal gland. Fluoride toxicity can lead to renal damage in children. Researchers studied 210 children living in areas of China with varying levels of fluoride in water (0.61–5.69 ppm). Among this group, the children drinking water with more than 2 ppm fluoride – particularly those with dental fluorosis – were found to have increased levels of NAG and y-GT in their urine, both of which are markers of kidney damage. The children’s urine also contains increased levels of lactic dehydrogenase – a possible indicator of liver damage. A diseased kidney is unable to effectively excrete fluoride, so individuals with compromised kidneys are at risk of developing fluorosis even at normal recommended limit of 0.7–1.2 ppm.
Fluoride has been found to be mutagenic by causing chromosome damage and interference with the enzymes involved with DNA repair in a variety of cell and tissue studies carried out in animals. Recent studies have also found a correlation between fluoride exposure and chromosome damage in humans. The only government-sanctioned animal study to investigate whether fluoride causes cancer, in 1990, found a dose-dependent increase in cancer in the target organ (bone) of fluoride-treated, male rats. This led to a 14-year study carried out by Harvard University that showed a significant link between fluoridation and a rare form of bone cancer called osteosarcoma in young boys, consistent with the results of the 1990 animal study.
Fluoride as a neurotoxin has been proven in several animal studies. For example, a 2024 study found a predominance of Ca2+-permeable AMPARs in membranes and a shift between different NMDARs subunits in hippocampal cells of Fluoride–-exposed rats, which is typical for neurodegeneration and can at least partially underly the observed disturbances in cognitive capacities of animals and humans. Another 2024 study found that prenatal fluoride exposure to fluoride in the drinking water in Los Angeles was associated with increased neurobehavioral problems. A 2006 National Research Council report stated that it is apparent that fluorides have the ability to interfere with the functions of the brain and the body by direct and indirect means. This finding was confirmed by a study where groups of children exposed to 8 ppm fluoride in water were found to have lower average IQs, less children attaining high IQ, and more children affected by low IQ. While 8 ppm is much higher than the fluoride level added to water in fluoridation programs (0.7–1.2 ppm), these results are in congruence with previous studies from China indicating that fluoride may affect IQ at lower levels.
A recent systematic review conducted by the National Toxicology Program reported “with moderate confidence that higher fluoride exposure…is consistently associated with lower IQ in children.” The 2023 report also highlighted the lack of US studies investigating associations of fluoride exposure with neurodevelopment or cognition and stated that US studies would be valuable.
If fluoride is added to water which contains aluminum, then aluminum fluoride complexes will form. Aluminum fluoride complexes have the potential to interfere with many hormonal and some neurochemical signals. Aluminum fluoride was recently nominated by the Environmental Protection Agency (EPA) and National Institute of Environmental Health Sciences as a “high health research priority” due to its “known neurotoxicity.”
Let’s stop our reactionary, binary thinking, listen to scientists, not physicians who are not trained to be scientists or analyze scientific data (most physicians spend an hour or two each week reading medical literature, not scientific studies), and take action on the chemicals, including fluoride, in our food supply and drinking water. Remember, it’s the lifetime of exposure (our exposome) to chemicals that causes most of our diseases.
Witnessing the end of empire. The USA had a good ride from the 1930s until the 1980s, while the last 40 years has seen the beginnings of the end of empire. We are now in the acute phase of decline, and becoming what Britain became, a beligerent plutocracy that is a hollowed-out shell of its former self. There’s still time to save us, but we must act fast.Plutocracy that began in the 1980s under Reagan must be dismantled and a representative democracy restored.
“If you are someone who was able to overlook the genocide and cast a vote for Kamala Harris, then you already understand how a conservative was able to overlook Trump’s extremism to vote for him.” Meg Indurti, Los Angeles, CA
Palestine: The result of “democracies” in the USA and Israel. Someone please awake the USA from its 40 years slumber.Aka: How the wealthy pummel and control the people.
The middle-class has severely retracted since the 1980s, and real wage increases for working people have been flat for 40 years. Price and Edwards calculate that the cumulative tab for the four-decade-long experiment in radical inequality in the USA had grown to over $47 trillion from 1975 through 2018. At a recent pace of about $2.5 trillion a year, that number now has crossed the $50 trillion mark by 2020. In other words, the wealthy have extracted $50 trillion from the middle class over the last 50 years, with the extraction worsening over recent years. For example, remember when George W. Bush destroyed the economy from 2001-2009, allowing the rich to extract gobs of money from the middle class, and then Obama had to save the economy? To save the economy, Obama bailed out the wealthy using money from the middle class.
But many people in the USA middle class don’t understand why they’ve become poorer. And most don’t want to hear it. They’re in denial. The mainstream media in the USA promotes the denial. Young people find it harder and harder to buy a home and attain higher education, and those from the middle-class with higher education are the drivers of innovation and new businesses. As an example, UC Berkeley, the world’s best public (and affordable) college, graduates the largest number of entrepreneurs in the US. Berkeley and other world-leading colleges in California are a key reason why California is the innovation hub of the planet. And it’s part of the reason why California has the 5th largest economy on the planet (that fell to #10 under Republicans). As much as the rich conservative man and their shills, such as Reagan, tried to kill our public univesities, the people of California prevented them from doing so. But huge student debt on the middle class did arise. More of Reagan’s attack on the middle class. And why are homes so expensive now in the USA, including California? Reagan financialized housing, and now, for example, private equity owns many of the homes in CA, including in San Diego. And in our deregulated, privatized USA, the wealthy use algorithms to commit price fixing in the housing industry. Corporations, such as RealPage in Texas, offer these services to the wealthy. Many of the wealthy will do anything to make a buck. Anything. Cast your eyes on Palestine, and you’ll know what I mean.
We will be targeted once again by Trump, and given his guard raills have been weakened by the “Supreme” Court, guarding our institutions in California will be hard during these next 4 years.
The Reagan Revolution
Despite what Ronald Reagan’s handlers, self aggrandizing plutocrats, told him to say, government is the solution to most, if not all, problems. Saying that government, the power of the people in a democracy, is the problem, was a damnation of democracy by Reagan. Without proper democratic regulations, “free markets” (there is no such thing as a free market) become unstable and often crash – such as the Savings and Loan Crisis that Reagan ushered in, and the rich become richer. Reagan’s Neoliberalism would gut the middle class and manufacturing, and lead to a government run by plutocrats. Essentially, Reagan would make the government an enemy of the people, and then blame the government for gutting the people. Stupid people believed him, rich people prospered. To bring plutocracy to the US, Reagan would even commit treason by cutting a deal with Iran to block President Carter from bringing back the US citizens held hostage in Iran, thus diminishing Carter’s bid for reelection. The Republican plutocratic strategy works by persuading white working class voters to focus not on financial self-interest, but on race, conservative religious values and other perceived identity threats, and this blights the US economy. The national debt soared 3X under Reagan and the US moved from a creditor nation to a debtor nation. Other people’s money, taken from the middle class, fueled the Republican ideology of making the rich even richer. Reagan’s privatization and deregulation of healthcare, including for example, an FDA where the clinical trials are run by companies and half of the budget of the FDA comes from the companies being regulated, would lead to the medicalization of America and the world’s worst and most expensive healthcare system. As governor, Reagan would cut one of the most important things driving the innovation in California, the great public universities in the state. All of this meant that Reagan was moving money away from innovation and the public good, and into the hands of the wealthy. Later, the Reagan Revolution-Republicans would kill government funding of new technologies, sending lithium ion battery technology and solar technology to China, leading to the Chinese domination of these markets. While the Reagan-Republicans embraced ignorant private enterprise ideologies that have never worked, not in the history of mankind, and failed to back US developed technologies – the Chinese knew Reagan-Republicans wouldn’t back US developed technologies and took great advantage of decades long research and development in the US, buying US technologies for pennies on the (thousands) dollar. Dwight D. Eisenhower rolls in his grave.
Diminished R&D in the USA
And as the wealthy pay little or no taxes, and with Trump exacerbating the already huge problem, the government no longer has the money to drive innovation – government has been and continues to be the main driver of innovation. Think about it, the vacuum tube, the semiconductor, the 3-dimensional transistor, RISC computer achitecture, solar panels, lithium ion batteries, rocket technology, airplane technology, nuclear imaging, almost all of our drugs, including new cancer treatements, the internet, CRISPR, etc, were government innovations. Without innovation, businesses are not created to monetize that innovation. Decreased R&D by the US government is why the Chinese have surpassed the US in many areas of science and technology, including AI, and their economy has flourished like nothing else before it (not even the US so rapidly built an economy). Like in Rome, where the wealthy built colliseums to placate the people, so too does the USA build more and more stadiums to placate the masses. And it makes the billionaires even wealthier. What’s happening?
The USA Repeats the UK Downfall Scenario
History repeating. Between 1880 and 1920, Britain killed 100 million Indians. Empire was at its peak. The rich were drinking all day, enjoying drunkeness at their huge estates, including in India. Like many other “English gentlemen” of the day, Winston Churchill’s father had spent his fortune on booze and other indulgences and had to marry a rich US citizen to save his estate and way of life. Winston world carry on dad’s ways – a drunkard he was of first class. The drunkards would then start two world wars, declaring war on Germany twice – wars they could never win without enlisting the Americans to win the wars for them. Eisenhower led the Allied forces while Winston drank and made belligerent speeches. Today these types of rich people often use ketamine and make speeches that reflect something other than reality. After the big war, Winston, a huge bigot, would go on to wreak havoc in the Middle East. Overthrowing the democratically elected president of Iran (with the help of Israel and the CIA) and starting a war with Egypt (Eisenhower wouldn’t particpate in this nonsense), are just two examples. An austere, conservative UK government would support the wealthy, ignore the middle-class, and gut R&D. Even its once venerated National Health Service is in steep decline. Sound familiar? (The drugs don’t work because Reagan privatized clinical trials – hopefully RFK Jr can do something about this huge, costly problem). Today the UK is a place where little works and the country has fallen to 3rd world status, especially after having iniated the conservative’s plan of Brexit. Trump supported it of course and has iniated a form of it in the USA. History repeating.
Trump promises more privatization and deregulation, something that brings about corruption, inefficency, inferior products, and higher prieces, following what began in the 1980s by Reagan to benefit the wealthy. Reagan so disdained the middle-class that he instituted taxes on their social security income. Financialization of the housing market began in the 80s, and housing costs skyrocketed. The Savings & Loan crisis brought about by deregulation was part of the problem. The problems continue and worsen today. Even our “cherised and abandoned” military has suffered from privatization and deregulation. As explained by Col. Wilkerson, US weapons are now worse than those from Russia and China and cost three times as much. Price gouging is the rule. Before the Reagan era (error) we witnessed President Kennedyend price gouging by large corporations through direct action. As a result, the price gouging stopped. Those days are gone. Corporations own our politicians (except bernie). Companies such as Boeing are now a joke, having been cannabalized by the wealthy. But the rich become richer (yes, Reagan deregulated stock buybacks to allow the rich to become richer) and the middle class pays. And, of course, the poor people die, or, if they’re lucky, become indentured servents.
“We’re not going back!” Sorry, we went back in the 1980s, never to return.
Lewis “Corporations Are People” Powell, architect of the “Going Back Movement” where Robber Baron 2.0 started. Back in 1971, when the Robber Baron memo was prepared, Powell was a well-connected partner in the Richmond-based law firm of Hutton, Williams, Gay, Powell and Gibson and sat on the boards of 11 major corporations, including the tobacco giant Philip Morris.
The 50 Year Republican Plan to Implement a Plutocracy
What we’re witnessing in the USA is the fulfillment of a 50 year plan. Lewis Powell laid it out in 1971 during the Nixon presidency, and every year hence, Republicans have followed it. Many Democrats have embraced it too. Look at the genocide in Palestine. Wealthy donor money from the Israel Lobby to both parties fuels the mass murdering of the innocents, as the invading Russians and Polish, such as PolakDavid Grun (aka Ben-Gurion) and Russian Moshe Sharett, setup, maintain, and expand their colonial, apartheid state in Palestine. Zionists laid down modern-day terrorism, something they learned from the British, in the Middle East. The citizens of the USA don’t support the genocide, but given no democracy in the USA, the wealthy donors are given what they want. Biden gives the genocidal maniacs all the weapons they want, receives millions in return, and Trump tells the genocidal maniacs to “finish them [Palestinians] off.” With a $100 million in his pocket from Israeli Zionist Miriam Adelson, Trump backs Polak, Benjamin Mileikowski’s (aka Netanyahu) plans for further stealing of Palestine’s land. Wealthy defense corporations and their senior leadership and owners are making a bundle by mass murdering innocent people. As Israel’s oldest newspaper says, ethnic cleansing is at hand. The U.S. has spent at least $22.76 billion on military aid to Israel and related U.S. operations in the region between Oct 2023 and Oct 2024. What am I talking about here when I say wealthy donors?
The Powell plan was to turn the USA over to the richest men and the largest corporations. This was a plan to replace our weak democracy with oligarchy. Many of America’s richest people invested billions in this plan, and its tax breaks, deregulation, privatization, and fossil fuel subsidies have made them trillions. Deregulation and privatization gave us Enron as one of many examples. Money flowed to the wealthy at Enron in Houston, TX resulting in the bankruptcy of many small businesses in California. Now coming in 2025, even more will soon come to the wealthy.
As any advertising executive or sales guy, such as Elon Musk, can tell you, with enough money and enough advertising — particularly if you are willing to lie — you can sell anybody pretty much anything. Given a highly religious USA and most people without (only 37%) higher education, fooling the masses is easy. Colonizing Mars – it’s a billion dollar scam. FSD – same. Hyperloop– same. Tunnels in Vegas – ditto. I could go on. Bullshit pervades. To see how stupid people are who voted for Trump, watch this. Those with a few synapse functioning above their midbrain are regretting thier vote for Trump upon realizing they voted against their own interest.
The Pitiful Binary Choice for President of the USA -Which Corporate Shill Do You Prefer?
Even a convicted felon, liar, fraudster, rapist, and friend and agent of America’s enemies can and has succeeded. This is a guy who used the Presidency to self-aggrandize. On the other side, we had another bullshiter who couldn’t even tell the truth about where she was born and raised – Berkeley, CA. Her father, Prof. Dr. Donald Harris, Ph.D., a Berkeley-educated and preeminent econonmist at Stanford was nowhere to be found in her story. Why? Because post-Keynesian ideas to development economics are uncool in our new era of Neocon politics. We don’t help poor people, we take advantage of them. If the rich need to increase their profit margins and need cheap labor to make some fancy sneakers, enlist child labor in Asia. Middle-class jobs in the USA are lost and the great income divide worsens. It’s Reagan’s NAFTA legacy at work, and the Heritage Foundation is proud to have had a puppet in Ronnie. The Keynesian ideas were used in the days when the greatest builders of the US economy and the middle-class- Roosevelt, Eisenhower, and Kennedy, were loved by the people, but would now be labeled as communists by guys like Trump. Kamala appeared as a phony, and people don’t like phonies. Trump played himself- a dumb, arrogant, lazy, loud, beligerent, and boastful white guy, and uneducated religious people loved it. Trump didn’t listen to his consultants, and it paid-off. Roy Cohn, the tyrannical closeted gay Jewish lawyer had taught him well. Kamala listened, and was clobbered. Thirteen million demoralized Democrats stayed home on Nov 5, 2024. Democrats don’t like genocide, especially when we are the perpetrators. Politics makes for strange bedfellows in our Neocon era, and most of these dogs come away flea-infested.
America was overwhelmed this fall by billions of dollars in dishonest and misleading advertising, facilitated by five corrupt Republicans on the Supreme Court, and it worked. Democrats were massively outspent, not to mention the power of the billionaire Murdoch family’s Fox “News” and 1500 hate talk radio stations. And third-party candidates, or candidates not selected by the donor class within the corrupt political processes of the two party system, were excluded by the wealthy donors. If you don’t cater to the rich man wishes, you don’t politically exist. You’re dead.
More broadly, and we find that corruption goes way beyond just this election; many of the crisis the USA is facing now are either caused or exacerbated by the corruption of big money authorized by five corrupt Republicans on our Supreme Court.
They are responsible for our crises of gun violence, the drug epidemic, homelessness, political gridlock, the houses being wiped-out in Florida by hurricanes and flooding, our slow response to the climate emergency, a looming crisis for Social Security and Medicare, the situation on our southern border, that most drugs don’t work (hopefully RFK, Jr will exert positive results on this problem), even the lack of affordable drugs that do work, insurance, and healthcare.
Billionaires Choose Our Supreme Court Too
All track back to a handful of Supreme Court justices who were handpicked by billionaires and who’ve sold their votes to billionaires in exchange for extravagant vacations, luxury yachts and motorhomes, private jet travel, speaking fees, homes, tuition, and participation in exclusive clubs and billionaire networks that bar the rest of us from entry.
For over two decades, Clarence Thomas and his wife have been accepting millions in free luxury vacations, tuition for their adopted son, a home for his mother, private jet and megayacht travel, and entrance to rarified clubs.
Sam Alito is also on the gravy train, and there are questions about how Brett Kavanaugh managed to pay off his credit cards and gambling debts. John Roberts’ wife has made over $10 million from law firms with business before the court; Neil Gorsuch got a sweetheart real estate deal; Amy Coney Barrett refuses to recuse herself from cases involving her father’s oil company.
None of this is illegal because when five corrupt Republicans on the Court legalized members of Congress taking bribes they legalized that same behavior for themselves.
As a result, we have oligarchs running our media, social media, and buying our elections, while the Supreme Court, with Citizens United, even legalized foreign interference in our political process. Oil billionaires own many of our TV stations, for example.
Our modern era of big money controlling government began in the decade after Richard Nixon put Lewis Powell — the tobacco lawyer who wrote the infamous 1971 “Powell Memo” outlining how billionaires and corporations could take over America — on the Supreme Court in 1972.
In the 1976 Buckley v. Valeo decision, the Court ruled that money used to buy elections wasn’t just cash: they claimed it’s also “free speech” protected by the First Amendment that guarantees your right to speak out on political issues.
In the 200 preceding years — all the way back to the American Revolution of 1776 — no politician or credible political scientist had ever proposed that spending billions to buy votes with dishonest advertising was anything other than simple corruption.
The “originalists” on the Supreme Court, however, claimed to be channeling the Founders of this nation, particularly those who wrote the Declaration of Independence and the Constitution, when they said that “money is the same thing as free speech.” In that claim, Republicans on the Court were doing what they do best- lie.
In a letter to Samuel Kercheval in 1816, President and author of the Declaration of Independence Thomas Jefferson explicitly laid it out:
“Those seeking profits, were they given total freedom, would not be the ones to trust to keep government pure and our rights secure. Indeed, it has always been those seeking wealth who were the source of corruption in government.”
But Republicans on the Supreme Court weren’t reading the Founders. They were instead listening to the billionaires who helped place them on the Court in the first place. The wealthy had bribed them with position and power and then kept them in their thrall with luxury vacations, “friendship,” and gifts. In this way, the wealthy have the court to back-up their money-making schemes.
Two years after the 1976 Buckley decision, the Republicans on the Supreme Court struck again, this time adding that the “money is speech and can be used to buy votes and politicians” argument applied to corporate “persons” as well as to billionaires. Lewis Powell himself wrote the majority opinion in the 1978 Boston v Bellotti decision.
Justices White, Brennan, and Marshall dissented, writing:
“The special status of corporations has placed them in a position to control vast amounts of economic power which may, if not regulated, dominate not only our economy but the very heart of our democracy, the electoral process.”
But the dissenters lost the vote, and political corruption of everything from local elections to the Supreme Court itself was now assured. The large middle-class was an annoyance to the wealthy as their power was being questioned by the newly educated middle class. All that was needed was a small middle-class to manage the wealth of the powerful – all other middle-class people needed to be purged so as not to upset the accumulation of wealth at the top. As so it began.
Notice that ruling came down just two years before the Reagan Revolution, when almost all forward progress in America came to a screeching halt. The Reagan Revolution had been primed, and the age of greed fell upon the USA for the next 40 years.
And it’s becoming worse. The Court doubling down in 2010 with Citizens United, overturning hundreds of state and federal “good government” laws dating all the way back to the late 1800s.
Thus, today America has a severe problem of big money controlling our political system. And last night it hit its peak, putting an open fascist in charge of our government. Granted the alternative was not good, but the greater of the two evils won, bigly.
The USA is an Outlier
No other developed country in the world has this problem, which is why every other developed country has a national healthcare system, free or near-free college, and strong unions that maintain a healthy middle class. Their streets aren’t strewn with the homeless. It’s why they can afford pharmaceuticals, are taking active steps to stop climate change, and don’t fear being shot when they go to school, the theater, or shopping.
It’s why they still have functioning democracies.
The ability of the USA to move forward on any of these issues is, for now, paralyzed with the election of Trump and the GOP taking over the Senate, and likely the House.
This is not the end, though; hitting bottom often begins the process of renewal.
Many citizens of the USA who are cognizant of the problems that began with the Reagan Revolution will continue to speak out and fight for a democracy uncorrupted by the wealthy donor class. I will do my part too.
The cofounder of SpaceX, aerospace engineer Tom Mueller (BS and MS in engineering), and his team, who developed the now successful SpaceX technologies, have left the company. What’s left is an insel with a speech impediment pretending to be an engineer and who thinks he’s an engineer because he takes credit for other people’s engineering work. He pretends (here are the real founders) to be a founder of Tesla to look cool. At least his good buddy, Peter Thiel is gay, and doesn’t have to worry about how to get a girl. And now he’s created the downfall of SpaceX, the Starship. If Sigmund Freud were alive today, he’d have a field day with Starship and Musk’s obsession with sex. Thanks to the deregulation and privatization of government, including NASA, a woman at NASA who chose to fund Starship, was then hired by SpaceX with a big salary. It’s called regulatory capture, and it’s a key reason, along with reduced government funding of R&D, why the US is falling behind in the science and technology race, including the space race where China may soon lead.
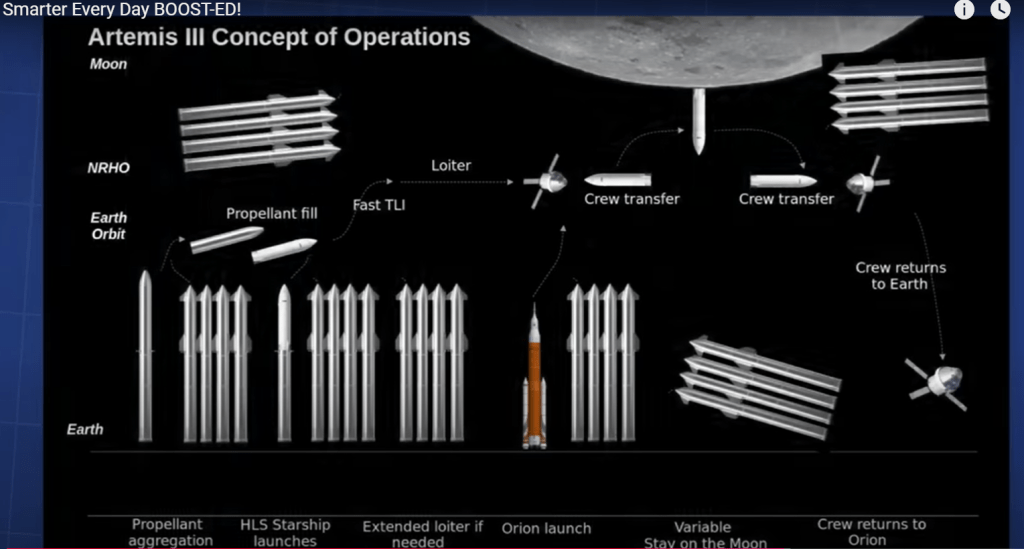
Starship is a complicated mess of a project requiring about 20 Starships to land one lunar module on the moon. Look at Thunderfoot’s video on the project for a deep-dive into more of Musk’s tomfollery. Scientists and engineers in Germany have published a paper on the infeasibility of a Starship mission to Mars. The below image is an outcrop of the video schematizing just how fanatstical is the Starship boondoggle that will never go to the moon.
Colonizing Mars is a bad joke. As the deregulated and privatized capital (money) of the USA is flowing to the billionaires who want to look cool by saying outlandish things such as we can colonize Mars with our current technology, the science and technology of the USA continues to diminish as we hand over our lead to China. Some people are finally catching-on to what’s happening to our country the 40 years hence that Ronald Reagan handed over everything to the plutocrats. Shit, we can’t even colonize the deserts on Earth, which are a veritable cornucopia compared to Mars.
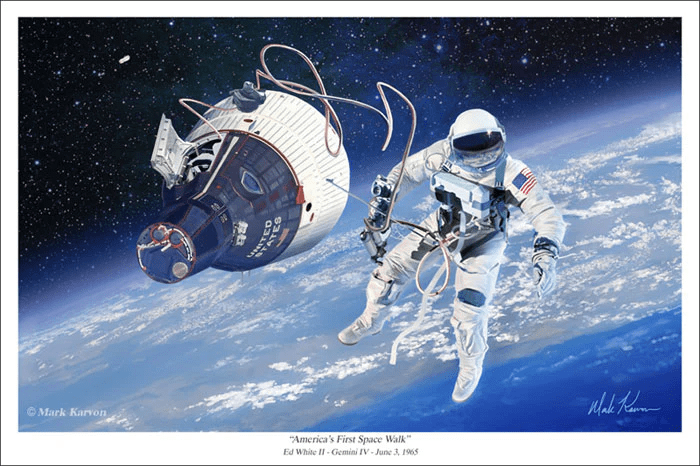
A picture of the billionaires who did a space walk during a SpaceX mission in 2024. Oh, wait a second, that’s a picture of NASA’s space walk in 1965, where, unlike SpaceX in 2024, the astronaut, Ed White, actually left the spaceship and “walked” in space.
The rich have taken over politics, do everything they can to make government look bad, and then tell the US middle class how bad the government is, having themselves made the government awful. Then the wealthy lobby and pay-off politicians, using the government doesn’t work mantra, to pass laws that deregulate and privatize government. Deregulation means the wealthy can do what they want. And privatization means the wealthy capture taxpayer’s dollars. Who cares if Tesla and SpaceX are polluting Texas. Pollution is the greatest cause of disease, but the rich guys don’t care. This deregulation allows the wealthy to then further strip down the government and takover those government functions. Electricity, water, prisons, schools, internet, “public radio and TV (yes, Republicans privatized these too),” the military, roads, elections, you name it, it’s in the hands of the wealthy and their corporations. And they do what they want with little interference. Houston, Texas-based Enron was a great example, where the rich guys in Texas did everything possible to hurt middle-class Californians. Want to send yourself into space along with some billionaire buddies, go ahead, the US middle class will pay for your folly. Hell, some of these middle-class morons will actually storm the US Capitol Building, break-in, and kill the Capitol Police, in defense of the plutocrats stealing wealth from them, the middle-class.
Meanwhile, the Chinese use their capital to build the world’s greatest science and technology. and they’re beating us on the moon and mars. China does not have a insel with a speech impediment leading their space program, instead they have an engineer leading their program.
SpaceX recently accomplished, well, almost accomplished, what NASA did back in 1965. Nearly 60 years ago, a man, NASA astronaut Edward White, exited the spaceship and floated around space on a tether back in ’65. Those were the days in the USA when science and scientists were valued. Scientists such as Dr. Thomas Paine, Ph.D., led NASA. But now, the privatized SpaceX and its billionaires couldn’t even accomplish in 2024 what NASA did in 1965. Instead, the SpaceX billionaires popped their heads outside the hatch and had a quick look while still in their space capsule. And, congratulations to the US middle class taxpayers, you’re hard earned dollars support these billionaires in their playtime in space.
SpaceX fails to accomplish what NASA did in 1965, but uses taxpayer dollars to give billionaires a joyride in orbital space.
Considering the SpaceX catch of the booster rocket for Starship, a miraculous feat, right?Here’s a picture ot it:
Oh, wait a minute. That’s the McDonnell-Douglas DC-X, known as the Delta Clipper, performing a precise reentry to the launch pad back in 1993. Another company, Astrobotic, has had reusable vehicles for years with the most rocket-powered return-to-pad-landings in the industry, not to mention the reusable Space Shuttle in the 1970s. Here’s Dr. Philip Mason, Ph.D., a chemist, take on the SpaceX Starship program and the reentry of the booster. Then there is Masten Space Systems – Masten has demonstrated more than 600 successful flight operations across five vertical takeoff and vertical landing vehicles beginning in 2009.
For a bigger waste of money, according to current estimates by scientists and engineers, a single Starship may need 20 other Starship launches to gather enough fuel through a complex refueling strategy in orbit to reach the Moon. NASA spelled-out the what a ridiculous plan is Starship for going to the moon, or beyond, in a 2023 report. Refueling will occur in low Earth orbit – so imagine the pollution that will take place during refueling due to the high number of launches and the anticpated failure of SpaceX to accomplish this task. Lots of launches and the resulting atmospheric pollution, along with the leakage of methane and other propellents that will likely spill during the sloppy and/or failed refueling attempts. You think global warming is bad now, just wait until Musk finishes off human life on the planet with his childish Buck Rogers fantasies.
In a presentation at a meeting of the NASA Advisory Council’s human exploration and operations committee Nov. 17, 2023, Lakiesha Hawkins, assistant deputy associate administrator in NASA’s Moon to Mars Program Office, said the company will have to perform Starship launches from both its current pad in Texas and one it is constructing at the Kennedy Space Center in order send a lander to the moon for Artemis 3.
SpaceX’s concept of operations for the Starship lunar lander it is developing for the Human Landing System (HLS) program requires multiple launches of the Starship/Super Heavy system. One launch will place a propellant depot into orbit, followed by multiple other launches of tanker versions of Starship, transferring methane and liquid oxygen propellants into the depot. That will be followed by the lander version of Starship, which will rendezvous with the depot and fill its tanks before going to the moon.
Florida has an economy built on rebuilding from hurricances and floods, fraud of all kinds, retirees, and tourism.Led by a corrupt governor, it’s a deregulated mess and falling down, fast.Conservative media that ballyhooed Miami as “Silicon Valley South” is media hype as the one and only large VC firm with offices in Miami pulls out after two years of non-action as the dream of a Miami tech hub is dead.
In the land that time forgot, led by a regressive, corrupt mafioso, DeSantis, once again Florida is #1 in healthcare fraud. South Florida is where medical equipment scams involving knee and back braces continue to flourish alongside more sophisticated billing schemes in the expanding field of telemedicine and genetic cancer testing. Florida is #2 in consumer fraud. The “Scumshine State” with so many people leaving the state, has exported it’s fraud to neighboring Georgia, which is now #1 in fraud with Florida at #2. Credit card fraud, guess who’s #1. Elder fraud, Florida got’s you covered. Corporate Ponzi schemes, Florida’s the place. Anything goes in Ron DeSantis’ deregulated Florida. Illicit drug money flows into the state, where money is often laundered in condos that will eventually collapse into the ocean. Drug money and money laundering makes for big buildings that obscure the views of the ocean, but the flooding running into you condo makes you realize that it’s there. As Florida floods, the raw sewage flows into whats left of people’s homes. The sewage is everywhere. And in Florida, they just keep building in flood prone areas. Florida is the land where climate science is ignored by the Republican-led government, but felt by the people. Oil tycoon money rules in Florida. I could go on, but you get the idea.
And Florida’s tech scene, the little that is present, is crashing. Why? There is a lack of talent and the elite universities that train talent, such as found in California, for instance at UC Berkeley, New York, and Massachusetts. Florida’s colleges are second rate and falling fast. VC funding in Florida is crashing. Right wing idiots like DeSantis are ruining the state’s college system. New College is fully destroyed. Others are crumbling. The state is dumbing down. The new curriculum in Florida is White Nationalism. Florida, especially Miami, is the land of tech fraud, biotech fraud, physician biotech fraud, and especially crypto fraud, along with nearby Bahamas, the home of FTX. Florida’s tech scene is a joke.
If your moving to Florida for it’s tech scene, move for the hurricanes and stay for the fraud – you’ll find little else. Like the state itself, the coral reefs in Florida are 90% destroyed. And….don’t forget your wading boots, because the cities are frequently underwater.